Dual Pathway Inhibition in Chronic Stable Coronary Artery Disease for the Prevention of Secondary Events
Matthew C Becker, MD FACC FSCAI FSVM Molly Mraz, BS (‘22)
Director, Cardiac Catheterization Laboratories Department of Biology
Chairman, Structural Heart Therapies University of Richmond
The Saint Vincent Heart and Vascular Institute Richmond, Virginia
Allegheny Health Network
Erie, Pennsylvania
Background
Patients with stable atheromatous disease of the coronary or vascular beds remain at high risk of secondary events despite aggressive use of antiplatelet therapy. The combination of vitamin K antagonists and antiplatelet agents has historically been met with unacceptably high risk of bleeding. Prolonged dual antiplatelet therapy (DAPT) modestly reduces cardiovascular events but also at the cost of bleeding. Recent data demonstrates that the novel combination of low-dose rivaroxaban in conjunction with low-dose aspirin can dramatically reduce the combination of cardiovascular death, myocardial infarction (MI), and stroke with minimal excess bleeding.
Case Report
A 68-year-old man with a prior history of hypertension, hyperlipidemia, type 2 diabetes, and prior tobacco abuse presents to the outpatient clinic for a routine follow-up after receiving 2 drug-eluting stents (DES) to the left anterior descending coronary artery in the setting of stable ischemic coronary artery disease (CAD) 6 months prior. The intervention was uneventful without complication. It rendered the patient free of all anginal symptoms and he was able to discontinue isosorbide mononitrate and ranolazine as a result. He has intensified his lifestyle modification efforts and as such, has reduced his hemoglobin A1C to 6.4. His most recent lipid profile demonstrates an LDL cholesterol of 86 mg/dL, and triglycerides of 207 mg/dL. A basic metabolic panel obtained by his primary care doctor last week showed a creatinine clearance of 87 mL/min. He has remained faithfully compliant with the prescribed regimen of DAPT which consisted of aspirin 81 mg PO daily and clopidogrel 75 mg PO daily. He has not suffered any untoward bleeding events and his complete blood count shows a hematocrit of 42 and a platelet count of 327. He remains tobacco free and has reduced red meat in his diet to twice a month and has adopted a low-carbohydrate regimen. A supervised cardiac rehabilitation exercise program has been completed and he is now enrolled in a local program 3 days per week. The patient is retired from the United States Postal Service and remains active in his local Rotary club. He continues to golf twice a week and is currently doing so without symptoms.
Physical exam:
Vitals: 137/82; HR of 75 beats per minute; O2 Saturation of 97% on room air.
He is a slightly obese well-developed Hispanic male. He is resting comfortably and has no evidence of a carotid bruit and/or jugular venous distention.
His cardiac exam is unremarkable with a normal S1 plus S2 and a regular rate and rhythm. No murmurs rubs or gallops are appreciated.
His lungs are clear to auscultation in all fields.
Abdomen does not have evidence of bruit and or pulsatile mass.
Vascular examination is notable for normal radial and dorsalis pedis pulses. No evidence of malperfusion to the digits and there is no edema.
Normal hair growth is seen in the pretibial regions bilaterally.
Femoral bruit is not appreciated upon auscultation.
Medications:
- Lisinopril 10 mg PO daily
- Aspirin 81 mg PO daily
- Rosuvastatin 10 mg PO HS
- Clopidogrel 75 mg PO daily
- Metoprolol tartrate 50 mg PO b.i.d.
- Pantoprazole 40 mg PO daily


Figure 1. (A) Severe coronary atherosclerotic disease affecting the proximal and mid LAD. (B) Successful percutaneous coronary intervention with a drug-eluting stent to the above lesions.
Discussion with the patient regarding his long-term secondary prevention efforts is had. In addition to lauding his compliance with dietary and exercise regimen, a review of his medication list is undertaken. Based upon the current guideline recommendations, it is advised that he increase his risk supra statin to 20 mg PO q.h.s. to achieve an LDL cholesterol of at least under 70 mg/dL. In addition, it is suggested that the patient add icosapent ethyl 2gm PO b.i.d. in order to reduce the triglycerides under 150 mg/dL. While his blood pressure is improved, it is recommended that the lisinopril is increased to 20 mg PO daily to achieve a goal of less than 130/85. It is reassuring that he has experienced no bleeding with regard to DAPT and it is recommended that at this point in time he discontinue the clopidogrel having satisfied the 6-month recommendation for DAPT following stable ischemic heart disease DES implantation. Based upon the recent FDA approval of low-dose rivaroxaban 2.5 PO b.i.d. in conjunction with low-dose aspirin, a discussion is had with the patient regarding how those data may apply to his circumstances. Based upon his medical comorbidities, his low bleeding risk, and notable reductions in cardiovascular morbidity and mortality, it is decided the patient will start rivaroxaban 2.5 PO b.i.d. in addition to his ongoing use of low-dose aspirin.
Discussion
Atherothrombosis, the catalyst for most acute ischemic events, is a well described phenomenon of rupture of a thin-capped atheroma in an arterial bed leading to exposure of the sub endothelial lipid-rich necrotic core resulting in obstruction of flow by thrombotic material with platelets and fibrin deposition.1 Due to this phenomenon, patients with atherosclerotic disease involving the coronary or peripheral vascular beds continue to suffer unacceptably high rates of morbidity and mortality despite utilizing low-dose aspirin for secondary prevention of events. Even with aggressive contemporary medical therapy, numerous series suggest 5 to 10% of patients with cardiovascular disease have recurrent events each year.2 These event rates can be upwards of 21% in patients with atherosclerosis involving multiple vascular beds.3 It has long been understood that aspirin conveys a 19% lower risk of major adverse cardiovascular events as compared to a placebo, and incremental benefit can be had by adding a vitamin K antagonist for secondary prevention after acute myocardial infarction – but this is associated with higher rates of major bleeding.4,5 Consequently, routine use of anticoagulation in conjunction with DAPT has not been recommended for this patient population. However, recent studies indicate that utilization of dual pathway inhibition with lower doses of the factor Xa inhibitor rivaroxaban in the setting of acute coronary syndromes significantly reduced the rate of cardiovascular death, myocardial infarction, and stroke (8.9% vs 10.7%; p=0.008) as well as death from cardiovascular causes (2.7% vs. 4.1%, P=0.002).6 These data strongly suggested that a reduction in atherothrombotic events could be achieved with the refinement of drug dosing and the proper patient population.
Ref: Modified from Venaraju S, et al. Clinical Nuclear Cardiology: State of the Art and Future Directions. 4th Ed Philadelphia, Mosby Inc. 2010.
Ref: Adapted from White H, Clin App Thromb Hemost. 2014:20(5):516-523.
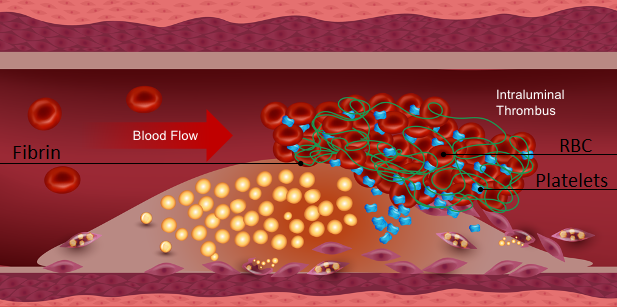
Figure 2. Non laminar blood flow resulting in rupture of a thin-capped atheroma subtending a lipid-rich necrotic core exposes potent pro coagulant sub-endothelial factors resulting in rapid generation of thrombin as well as aggressive platelet activation and propagation resulting in atherothrombosis with resultant obstruction of flow due to thrombotic material.
Subsequently, the COMPASS trial (Cardiovascular Outcomes for People Using Anticoagulation Strategies) randomized just over 27,000 patients with stable coronary artery disease (CAD), peripheral artery disease (PAD) or both to a regimen of rivaroxaban (2.5 mg twice daily) plus aspirin (100 mg once daily), rivaroxaban (5 mg twice daily), or aspirin (100 mg once daily) in order to assess a primary composite endpoint of cardiovascular death, stroke, or myocardial infarction. After a mean follow-up of only 23 months, the data safety and monitoring committee terminated the study early for superiority of the rivaroxaban 2.5 mg plus-aspirin group. This decision was driven by a robust 24% relative risk reduction in the composite end point (4.1 vs 5.4%, P=<0.001), but a statistical increase in minor bleeding (3.1 vs 1.9%; P=<0.001). Notable sub analyses indicate a significant reduction in all-cause mortality by 18%, reduction of cardiovascular death by 22%, and reduction of ischemic stroke by 42%. Of particular interest to the peripheral vascular community, an unprecedented and very significant reduction in acute limb ischemia of 44% was noted as well as a 70% reduction in major limb amputation.7

Modified from Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017;377:1319-30.
Figure 3. Dual pathway inhibition. Low-dose rivaroxaban reduces circulating serum levels of thrombin by inhibiting its production from prothrombin. Thus, decreased conversion of fibrinogen to fibrin predictably occurs resulting in anticoagulation. Decreased thrombin stimulation of the PAR-1 receptor results in a reduction of platelet activation and propagation. COX-1 inhibition via low-dose aspirin predictably results in antiplatelet effect. The combination results in a dual pathway inhibition which is the suggested mechanism for reducing atherothrombotic events in patients with polyvascular atherosclerosis.
Above we present a patient phenotype very commonly encountered in clinical practice that is prototypical of the COMPASS trial population. Historical data would recommend unequivocally the patient be managed with low-dose aspirin to mitigate secondary events as well as aggressively addressing the other modifiable risk factors such as hypertension, type 2 diabetes, and hyperlipidemia. While each of these comorbidities have innovative and guideline recommended therapies that can reduce morbidity and mortality, none have demonstrated the magnitude of benefit that was conveyed to the average patient in the COMPASS trial. On average, patients enrolled in COMPASS experienced a 24% relative risk reduction in the composite endpoint of cardiovascular death, MI, and stroke. While the above patient was not personally afflicted with PAD, the very notable reductions of acute limb ischemia and amputation (44 and 70% respectively) are unparalleled in historical and contemporary literature. Published in 1996, the CAPRIE trial (clopidogrel versus aspirin in patients at risk of ischaemic events) demonstrated that in a subpopulation of patients with symptomatic PAD, clopidogrel 75 mg daily was marginally more effective than aspirin 325 mg once daily in reducing the risk of a composite outcome ischemic stroke, MI, and vascular death (5.32% vs. 5.83% (RR 0.91; 95% CI 0.84-0.97; P=0.043).8 The combination of clopidogrel and low-dose aspirin therapy has also failed to meaningfully impact clinical outcomes in patients with stable cardiovascular and PAD – although a signal of benefit was seen in the subgroup with clinically evident atherothrombosis (relative risk, 0.88; 95 percent confidence interval, 0.77 to 0.998; P=0.046).9 Despite its superiority over clopidogrel in acute coronary syndromes, in a population of patients with symptomatic PAD, monotherapy with ticagrelor did not reduce cardiovascular event rates nor acute limb ischemia as compared to therapy with clopidogrel.10 Vorapaxar, a novel antagonist of protease-activated receptor-1, did significantly reduce the incidence of acute limb ischemia (2.3% versus 3.9%; hazard ratio, 0.58; 95% confidence interval, 0.39–0.86; P=0.006) and peripheral revascularization (18.4% versus 22.2%; hazard ratio, 0.84; 95% confidence interval, 0.73–0.97; P=0.017) as compared to a placebo in a population of patients with stable PAD. However, this did come at the cost of significantly increased major bleeding (7.4% versus 4.5%; P=0.001).11
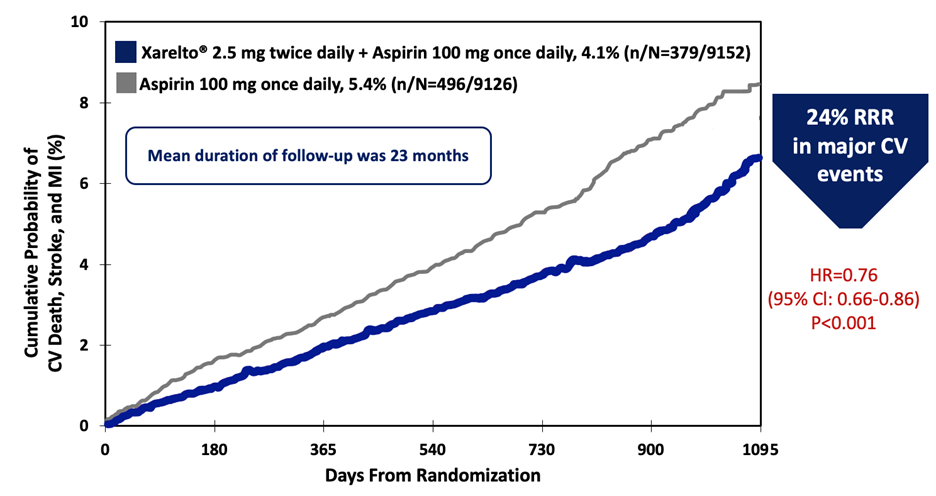
Figure 4. Kaplan Meier curves depicting ongoing and progressive reduction in events favoring the low-dose Xarelto + aspirin combination strategy culminating in early termination of the COMPASS trial at 23 months due to a significant 24% relative risk reduction in major cardiovascular events.
Modified from Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017;377:1319-30.
Furthermore, the dramatic reduction in ischemic stroke that was demonstrated in this population should be emphasized. While a small proportion of patients enrolled in COMPASS were known to have carotid or cerebrovascular disease, the rivaroxaban and aspirin treated population saw a 40% RRR in ischemic stroke as compared to the lone aspirin group. In order to add granularity to that finding, Sharma et al12 performed a subgroup analysis that revealed patients with a known prior stroke had substantially greater benefit from low-dose rivaroxaban and aspirin, having a 58% relative risk reduction as compared to the aspirin placebo group. This compares quite favorably with previously published data describing 32% relative risk reduction in recurrent events with the utilization of low dose aspirin and clopidogrel in the setting of acute ischemic stroke or transient ischemic attacks.13 Thus, substantial stroke reductions were seen in patients known to be at risk of ischemic stroke, and importantly, those without known cerebrovascular disease. This may well represent a future avenue towards primary prevention of ischemic stroke in the at-risk patient population.
Modest reductions in cardiovascular morbidity have been observed with prolonged DAPT after percutaneous coronary intervention (PCI). The DAPT trial long-term dual antiplatelet therapy versus placebo in patients who had received PCI and successfully tolerated 12 months of DAPT. Compared to the placebo, prolonged DAPT reduced the rates of stent thrombosis (0.4% vs. 1.4 P <0.001) and major adverse cardiovascular and cerebrovascular events (4.3% vs. 5.9 P <0.001). The rates of MI and death from any cause was also significantly reduced. However, this did come at the expense of an increase in moderate or severe bleeding (2.5% vs. 1.6%, P=0.001).14 The PEGASUS-TIMI 54 trial randomized patients with prior MI within the past 1-3 years to either Brilinta 90 b.i.d. or 60 b.i.d. with low-dose aspirin, and after 33 months, the median duration of therapy led to a significant reduction in cardiovascular death, MI, and stroke (7.85, 7.77, and 9.04 in the placebo group). This unfortunately came at the expense of significant increase in TIMI major bleeding – most notably in the 90 b.i.d. group (2.6 vs 2.3 vs 1.06). Thus, prolonged DAPT in a predominantly CAD intervention group modestly can reduce meaningful endpoints, however it does so at the cost of severe bleeding. Furthermore, recent trials have demonstrated low rates of thrombotic complications and low rates of major bleeding with truncated DAPT in high-risk bleeding patients presenting with an acute coronary syndrome (ACS).15 Thus, the ideal patient for prolonged DAPT remains somewhat unclear. In comparison, the more diverse and inclusive population enrolled in COMPASS not only generalized to a larger patient demographic, but also resulted in substantially larger reductions in cardiovascular death, MI, and stroke.7
Finally, major bleeding has been the Achilles heel of all prior attempts to combine systemic anticoagulation and antiplatelet therapies in an effort to reduce thrombotic events in patients with CAD.16 However, substantial past experience and further refinement of the characteristics of factor Xa inhibitor molecules has led to the current iteration of dual pathway inhibition as discussed above. As tested in the COMPASS trial, the current dosing regimen of rivaroxaban 2.5 PO b.i.d. in conjunction with low-dose aspirin 100 mg daily yielded a statistically higher rate of major bleeding by the modified ISTH criteria (3.1 vs 1.9%; p=<0.001). This was primarily driven by what is traditionally considered clinically relevant, but nonmajor bleeding events such as ecchymosis, epistaxis, and hemorrhoidal bleeding did not require hospitalization (1.1 vs 0.5; P=<0.001). Furthermore, Anand et al17 demonstrated that by applying the modified CART or REACH scores (poly vascular disease, heart failure, diabetes, renal insufficiency CrCl < 60mL/min) to further risk stratify the general COMPASS population, a substantially greater proportion of events can be prevented per 1000 patient years at the cost of only several major bleeds, depending upon the specific criterion employed. Therefore, the cost benefit analysis for utilization of this novel combination therapy can be individually applied to a physician’s own patient population.
Conclusion
Atherothrombosis remains a common and high-risk occurrence in many patients with atherosclerosis affecting the coronary and vascular arterial beds. The past decade has resulted in great progress in the application of pharmacotherapy to reduce the morbidity and mortality associated with this large and growing population. Despite these advances, rates of cardiovascular death, MI, and stroke as well as acute limb ischemia and amputation remain unacceptably high. Evidence from the landmark COMPASS trial suggests that the utilization of low-dose rivaroxaban in combination with low-dose aspirin through dual pathway inhibition can further significantly reduce these events with low rates of excess major bleeding.7
References
- Fuster V, Moreno PR, Fayad ZA, et al. Atherothrombosis and high-risk plaque: part I: evolving concepts. J Am Coll Cardiol 2005;46:937–954.
- Bhatt DL, Eagle KA, Ohman EM, et al. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA 2010;304:1350-7.
- Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 2017;135:726-779.
- Antithrombotic Trialists’ (ATT) Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849-60.
- Anand SS, Yusuf S. Oral anticoagulants in patients with coronary artery disease. J Am Coll Cardiol 2003;41:Suppl S:62S-69S.
- Mega JL, Braunwald E, Wiviott SD, et al. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med 2012;366:9-19.
- Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017;377:1319-30.
- CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996;348:1329-39.
- Bhatt DL, Fox KAA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med 2006;354:1706-1717.
- Hiatt WR, Fowkes FGR, Heizer G, et al. Ticagrelor versus clopidogrel in symptomatic peripheral artery disease. N Engl J Med 2017;376:32-40.
- Bonaca MP, Scirica BM, Creager MA, et al. Vorapaxar in patients with peripheral artery disease. Circulation 2013;127:1522–1529.
- Sharma M, Hart RG, Connolly SJ, et al. Stroke outcomes in the COMPASS trial. Circulation 2019;139:1134.
- Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11-19.
- Mauri L, Kereiakes DJ, Yeh RW, et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. N Engl J Med 2014;371:2155-2166.
- Mehran R, Baber U, Sharma SK, et al. Ticagrelor with or without aspirin in high-risk patients after PCI. Engl J Med 2019;381:2032-2042.
- Hamon M, Lemesle G, Tricot O, et al. Incidence, source, determinants, and prognostic impact of major bleeding in outpatients with stable coronary artery disease. J Am Coll Cardiol 2014;64:1430–1436.
- Anand SS, Eikelboom JW, Dyal L, et al. Rivaroxaban plus aspirin in relation to vascular risk in the COMPASS trial. J Am Coll Cardiol 2019;73:3271-3280.