The High Cost Of Peripheral Artery Disease And Critical Limb Ischemia
Abstract
Despite the high prevalence of peripheral artery disease (PAD), this chronic disease continues to be underestimated, underdiagnosed, and undertreated. PAD is frequently ignored or dismissed as “a lifestyle disease.” Underdiagnosis and undertreatment result in high patient morbidity and mortality. Coronary and cerebrovascular disease are major contributors to this morbidity and mortality. The economic burden of PAD is significant, exceeding that of many other common chronic diseases. Earlier diagnosis and appropriate treatment of leg symptoms, as well as comorbid cardiovascular disease and diabetes, could reduce the economic cost.
Peripheral Artery Disease Prevalence
In 2015, the prevalence of PAD was almost 20 million.1 Comparing this number with the U.S. prevalence of other chronic diseases, only diabetes (36 million) is more common.1,2 In comparison, stroke has a prevalence of 7.2 million.3 Even coronary heart disease (CHD) and all cancers afflict fewer U.S. individuals, at 16.5 million and 15.5 million respectively, than lower limb atherosclerotic disease.3,4 Despite the high rates of PAD, it frequently is not included in reviews of cardiovascular disease.5,6
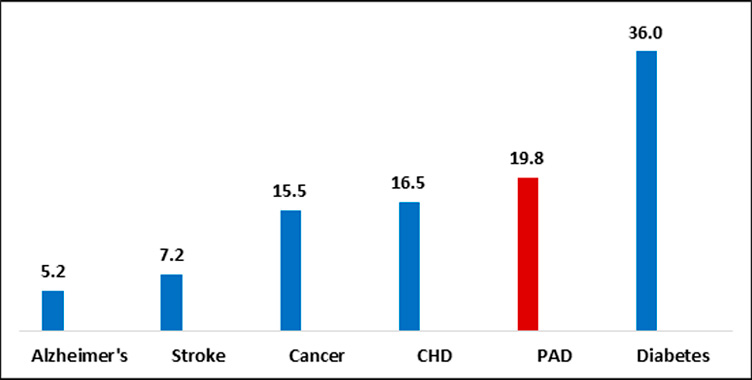
Source: Yost,1 Menke,2 Benjamin,3 American Cancer Society4 and Alzheimer’s Association.7
Economic Cost
In 2015, the total economic cost of PAD was between $224 and $414 billion.8 The lower figure represents annual per patient costs in the U.S. reduction of atherothrombosis for continued health (REACH) registry.9 The higher figure is the per patient cost in the Margolis managed care study.10
Reported costs in these two studies were inflated to 2015 dollars employing the appropriate medical care components of the U.S. consumer price index (CPI).11-13 Unless otherwise noted, all other cost data in this article has been inflated to 2015 dollars.
Both the REACH Registry and the managed care study included inpatient and outpatient medical costs.9,10 The key difference between the two studies reflects the inclusion of all-cause hospitalization costs in the Margolis study.10 In contrast, per patient costs in REACH were PAD and cardiovascular hospital costs only.9
Majority of Costs Are Inpatient
Hospital costs account for the majority (65%-88%) of PAD costs, or $147 billion in the REACH study and $363 billion in the managed care study.8-10 Two Medicare studies also found that nearly 90% of PAD treatment costs were inpatient.14,15
Since hospital costs account for a bit less than one-third of total U.S. healthcare expenditures, PAD hospital costs are 2-3 times the national average.16
Non-PAD costs account for a significant portion of hospital costs. In patients hospitalized for cardiovascular reasons, 43% of costs are non-PAD costs.9 However, if we examine all-cause hospitalizations, then non-PAD costs account for almost 90% of the total.10,14
Frequent Presence of Polyvascular Disease Increases Costs
Most PAD patients have polyvascular disease. According to REACH, just 30% of PAD patients have PAD alone. The rest have some combination with coronary artery disease (CAD) and cerebrovascular disease (CVD). Significantly, over 60% have CAD either alone, or in combination with cerebrovascular disease.17
Polyvascular disease increases the cost. In 2015, PAD alone cost about $11,300 per year, or about the same as PAD with CVD. Costs rise to exceed $15,000 in patients with both PAD and CAD. The highest costs are generated by PAD patients with both CAD and CVD, representing almost $20,000 per year.17
Medicare Pays for Majority of the Peripheral Artery Disease Bill
Medicare and Medicaid pay 80% of the PAD hospital bill. Reflecting the preponderance of elderly patients, Medicare alone pays 71%.18 In contrast, Medicare pays 46% of the national hospital bill, with Medicare and Medicaid combined accounting for 60%.19
In the 2003-2012 period, between 10%-21% of Medicare patients were treated for PAD.20,21 The average expenditure per patient in 2015 dollars was between $22,756 and $72,159.8,14,15 This range reflects the definition of PAD, as well as the types of treatments included in the studies. Importantly, the higher number includes long-term care costs, as well as emergency and other services.15
Medicare spending of $72,159 per PAD patient is 6 times higher than the spend on an average beneficiary, $11,951.8,15,22
Economic Burden of Peripheral Artery Disease Exceeds Other Chronic Diseases
Comparing the cost of PAD to other chronic diseases, the economic burden is high and exceeds that of diabetes, CAD, and all cancers combined.3,4,8,23
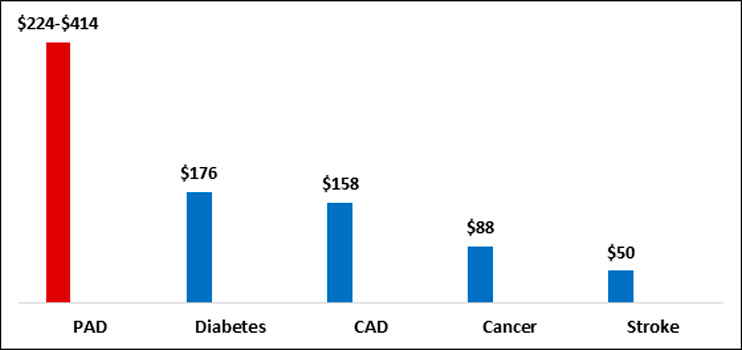
Source: Benjamin,3 American Cancer Society,4 Yost,8 Mahoney9 and American Diabetes Association.23
The $176 billion cost of diabetes represents the direct cost of the disease in 2012.23 Recently published data found that, by 2017, costs had increased to $237 billion, or $16,752 per patient.24 If we conservatively compare 2015 PAD costs to 2017 diabetes costs, the economic cost of PAD at $224-$414 billion is at least as high as diabetes and likely higher.
Critical Limb Ischemia Prevalence
Between 2.0 and 3.4 million of those with PAD have critical limb ischemia (CLI), the most severe form of the disease.1 These figures represent prevalent disease, not the number diagnosed and treated. Only a fraction, or approximately 700,000 to 800,000, are treated with revascularization or amputation.25
Cost of Critical Limb Ischemia
The cost of treating incident CLI cases in Medicare has recently been estimated at $4.2 to $12.0 billion.26,27 However, all-cause costs of prevalent disease in all age groups are considerably higher, estimated at $220 to $300 billion.28 The difference in the above cost estimates reflects the fact that the higher numbers are based on prevalent cases (3.4 million) in all ages rather than incident disease in Medicare. In addition, the costs to treat cardiovascular disease, diabetes, and all other comorbidities are included, which add significantly to the total economic burden.28
Factors Driving Up Costs
Interventional treatment of CLI is costly. In a recent analysis of Medicare CLI patients, 2016 costs per patient were $49,200 for surgical bypass, $49,700 for endovascular, and $55,700 for major amputation.27 However, interventional therapy is only one of many factors that increase the economic burden of CLI. Notably, these factors are all modifiable or preventable.28
Costs Increase with Disease Severity
Treatment costs for both PAD and CLI increase with disease severity. The inpatient cost of treating intermittent claudication (IC) in 2015 was $19,300. In contrast, the cost of treating CLI was almost $30,300.29 A recent German study also demonstrated that average inpatient costs for CLI treatment were higher than those for PAD patients in Rutherford Category 1-3.30
Within CLI, costs increase with severity of ischemia. Inpatient treatment of a patient with rest pain (Rutherford 4) costs approximately $24,000 and increases to $28,000 for a patient with ulcers (Rutherford 5). Inpatient costs for patients treated at the most severe stage, Rutherford 6, approach $40,000.26 German data also show a similar pattern of treatment costs increasing with increasing severity of CLI.30
These data suggest that earlier diagnosis and treatment at less severe stages of ischemia could reduce the economic burden of PAD and CLI.28
Diabetes
Age and diabetes are the key risk factors for CLI.31,32 Although age is not modifiable, the consequences of diabetes are with optimal glycemic control.33
Diabetes is an even stronger risk factor for CLI than it is for less severe lower limb disease. While diabetes increases the risk of PAD by 2-4 times, it increases the risk of CLI by 7-8 times.21,34-37
Diabetes is one of the major comorbidities in CLI. Whereas 14% of the general population is diabetic, approximately 60%-80% of the CLI population has diabetes.2,28,31 The co-prevalence of these two diseases has implications for CLI severity and morbidity, as well as for treatment costs.
Diabetics have more severe ischemia and are more likely to present with more severe disease, characterized by ulcers and gangrene.31,38,39 Critical limb ischemia develops suddenly in diabetics.40 Diabetics with CLI have more amputations and a 28 times higher risk of amputation.41-49 The risk of amputation increases with the severity of diabetes measured by HbA1c.50-52 The rate of amputation also increases with age.49 The presence of diabetes increases CLI costs.53-55
Polyvascular Disease
The majority of CLI patients have polyvascular disease.28 A recent study of Medicare patients found that almost half of CLI patients had CAD.27 Other studies in various CLI populations found that the prevalence of CAD was 48%-85%, while that of CVD was 16%-25% respectively.21,27,42,56-58 Approximately 20%-30% of CLI patients suffer from congestive heart failure (CHF).21,56,58,59
Cardiovascular disease (including hypertension complications) accounts for over 7% of CLI admissions. CHF represents 3.5% of CLI admissions, while myocardial infarction (MI) accounts for 1.84%.60 These cardiovascular hospitalizations and revascularizations add significantly to all-cause costs.28
Major adverse cardiac events (MACE) increase with disease severity, more frequently occurring in CLI patients than in those with IC.58 MACE is defined as nonfatal MI, nonfatal ischemic stroke, or cardiovascular death. Over half of deaths in CLI patients are due to cardiovascular causes.58 Despite this, CLI patients continue to be undertreated for their cardiovascular risk factors, even in comparison to IC patients.58,61,62
Suboptimal Risk Factor Management
PAD is considered a coronary artery disease risk factor equivalent. Recommended risk factor modification therapies include smoking cessation, aspirin, statins, and antihypertensives, as well as optimal glucose control in those with diabetes.61,63
Despite these guideline recommendations and the high prevalence of both coronary artery and cerebrovascular disease, CLI patients are undertreated for their risk factors.33,61 Statins, antiplatelets, and antihypertensives are underutilized. 33,61 Glucose is inadequately controlled in 40% of CLI patients and smoking persists in 29%-52%.33,36 Overall, only about one-third of CLI patients receive optimal medical management with all risk factor modification therapies. 33,61
Inadequate risk factor management increases both MACE and major adverse leg events (MALE). 33,61 One recent study concluded that suboptimal risk factor management increases the risk of amputation and/or death by 8 times. 33 The resulting adverse cardiac and leg events drive up CLI costs. The 2018 cost of MACE in CLI patients is conservatively estimated at $17.5 billion.28
Unplanned Readmissions
At 20%-27%, 30-day CLI readmissions are high and exceed the 12% rate for stroke and 15% rate acute for MI.26,29,64-67 At 6 months, almost 60% of CLI patients are readmitted. The majority of these readmissions are unplanned.26,64
All-cause readmissions are higher for CLI than for PAD and increase within CLI by Rutherford Category.26,29,67 For example, 30-day readmissions for gangrene are 25.0% versus 14.8% for rest pain.26
Significantly, less than one-third (21%-33%) of readmissions are due to primary CLI.26,64 The majority of readmissions are for non-CLI reasons such as procedure complications, infections, diabetes related non-vascular problems, and cardiovascular events. 26,64,65
High rates of unplanned readmissions increase CLI costs.26,65 A recent study estimated that, in 2016, CLI readmissions cost $624 million. The authors calculated that a 1% reduction in readmissions could save $15 million annually.26 Unplanned readmissions also increase MALE.68,69 Major adverse limb events add to the CLI cost burden.28,70
Most of the factors that lead to CLI readmissions are modifiable.68,71 Improved focus on prevention and early diagnosis and treatment of infection could reduce readmissions and associated costs.26 Meticulous surgical technique and peri-procedural monitoring could decrease procedure complications.65,68,71 Optimal cardiovascular risk factor management and diabetic care could decrease cardiovascular and diabetic readmissions. 65,68,71
Diagnosis and treatment of CLI at less severe stages could also reduce readmissions and costs. Since major amputation is a risk factor for CLI readmissions, replacing amputation with revascularization procedures could favorably impact readmission rates.28,64
Conclusion
While interventional therapy for PAD and CLI is costly, with primary major amputation being the most expensive interventional therapy, other primarily modifiable factors add to the economic burden of the disease. These include delay in diagnosis and treatment until the later stages of the disease, the high presence of polyvascular disease, suboptimal treatment of cardiovascular risk factors, and high rates of unplanned readmissions. Optimal management of risk factors and comorbid diseases (diabetes, CAD, CVD), as well as improved management of preventable issues like procedural complications and infections, could significantly reduce the economic burden.
References
- Yost ML. Critical limb ischemia. Volume I. Unites States epidemiology. 2016 Supplement. Beaufort (SC): THE SAGE GROUP; 2017.
- Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA 2015 Sep 8; 314(10):1021-9.
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart Disease and Stroke Statistics’ 2017 Update: A Report from the American Heart Association. Circulation. 2017 Mar 7;135(10):e146-603.
- American Cancer Society. Cancer facts and figures 2017. [Internet. Accessed 2019, Aug.] Available at: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdf .
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011 Mar 1;123(8):933-44.
- Nichols GA, Bell TJ, Pedula KL, O’Keeffe-Rosetti M. Medical care costs among patients with established cardiovascular disease. Am J Manag Care. 2010 Mar;16(3):e86-e93.
- Alzheimer’s Association, 2014 Alzheimer’s Disease Facts and Figures, Alzheimer’s & Dementia, Volume 10, Issue 2.
- Yost ML. The real cost of peripheral artery disease. Atlanta (GA): THE SAGE GROUP; 2011.
- Mahoney EM, Wang K, Cohen DJ, et al. One-year costs in patients with a history of or at risk for atherothrombosis in the United States. Circ Cardiovasc Qual Outcomes 2008;1:38-45.
- Margolis J, Barron JJ, Grochulski D. Health care resources and costs for treating peripheral artery disease in a managed care population: results from analysis of administrative claims data. J Manag Care Pharm 2005; 11(9): 727-34.
- Consumer price index (CPI). All urban consumers 12 month price change. Medical Care CPI. Series ID CUUR0000SAM. [Internet. Accessed 2019, May.] Available at: https://data.bls.gov/timeseries/CUUR0000SAM?output_view=pct_12mths.
- Consumer price index (CPI). All urban consumers 12 month price change. Hospital Services CPI. Series ID CUUR0000SEMD01. [Internet. Accessed 2019, May.] Available at: http://www.bls.gov/cpi/data.htm.
- Consumer price index (CPI). All urban consumers 12 month price change. Medical Commodities CPI. Series ID CUUR0000SAM1. [Internet. Accessed 2019, May.] Available at: http://www.bls.gov/cpi/data.htm
- Hirsch AT, Hartman L, Town RJ, Virnig BA. National health care costs of peripheral arterial disease in the Medicare population. Vasc Med 2008; 13: 209-15.
- Jaff MR, Cahill KE, Yu AP, et al. Clinical outcomes and medical care costs among Medicare beneficiaries receiving therapy for peripheral arterial disease. Ann Vasc Surg 2010;24:577-87.
- Centers for Medicare & Medicaid Services. National health expenditures 2015 highlights. [Internet. Accessed 2019 Aug. 28.] Available at: https://ccf.georgetown.edu/wp-content/uploads/pdfs/highlights.pdf.
- Mahoney EM, Wang K, Keo HH, et al. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ Cardiovasc Qual Outcomes 2010;3:642-51.
- HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. [Internet]. Available at http://www.hcup.ahrq.gov/
- Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2013. Statistical Brief #204 [Internet. Accessed 2019, Aug. 28.] Available at: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb204-Most-Expensive-Hospital-Conditions.jsp.
- Kalbaugh CA, Kucharska-Newton A, Wruck L, et al. Peripheral artery disease prevalence and incidence estimated from both outpatient and inpatient settings among Medicare
fee-for-service beneficiaries in the Atherosclerosis Risk in Communities (ARIC) Study. J Am Heart Assoc. 2017 May 3;6(5). pii: e003796. - Nehler MR, Duval S, Diao L, et al. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J Vasc Surg. 2014 Sep;60(3):686-95.e2.
- Hartman M, Martin AB, Espinosa N, Catlin A, The National Health Expenditure Accounts Team. National Health Care Spending In 2016: Spending And Enrollment Growth Slow After Initial Coverage Expansions. Health Aff (Millwood). 2018 Jan;37(1):150-160.
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2012. Diabetes Care 2013;36(4):1033-46.
- Riddle MC, Herman WH. The cost of diabetes care-an elephant in the room. Diabetes Care. 2018 May;41(5):929-932.
- Yost ML. Critical limb ischemia by Rutherford Category: prevalence and markets in patients and limbs. Beaufort (SC): THE SAGE GROUP; 2017.
- Kolte D, Kennedy KF, Shishehbor MH, et al. Thirty-day readmissions after endovascular or surgical therapy for critical limb ischemia: analysis of the 2013 to 2014 Nationwide Readmissions Databases. Circulation. 2017 Jul 11;136(2):167-176.
- Mustapha JA, Katzen BT, Neville RF, et al. Determinants of long-term outcomes and costs in the management of critical limb ischemia: a population-based cohort study. J Am Heart Assoc. 2018 Aug 21;7(16):e009724.
- Yost ML. The cost of critical limb ischemia. Why is the disease so costly? Beaufort (SC): THE SAGE GROUP; 2019.
- Martinez RA, Shnayder M, Parreco J, et al. Nationally representative readmission factors in patients with claudication and critical limb ischemia. Ann Vasc Surg. 2018 Oct;52:96-107.
- Reinecke H, Unrath M, Freisinger E, et al. Peripheral arterial disease and critical limb ischaemia: still poor outcomes and lack of guideline adherence. Eur Heart J 2015;36(15):932-8.
- Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD). TransAtlantic Inter-Society Consensus (TASC) Working Group. TASC document. J Vasc Surg. 2000;31:S1-S296.
- Jaff MR, Biamino G. An overview of critical limb ischemia. Endovascular Today 2004;3(2): 45-48.
- Chung J, Timaran DA, Modrall JG, et al. Optimal medical therapy predicts amputation-free survival in chronic critical limb ischemia. J Vasc Surg. 2013 Oct;58(4):972-80.
- Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res.2015 Apr 24;116(9):
1509-26. - Fowkes FG, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013 Oct 19;382(9901):1329-40.
- Howard DP, Banerjee A, Fairhead JF, et al. Oxford Vascular Study. Population-based study of incidence, risk factors, outcome, and prognosis of ischemic peripheral arterial events: implications for prevention. Circulation. 2015 Nov 10;132(19):1805-15.
- Baser O, Verpillat P, Gabriel S, et al. Prevalence, incidence, and outcomes of critical limb ischemia in the US Medicare population. Vascular Disease Management 2013;10:E26–E36.
- Jonason T, Ringqvist I. Diabetes mellitus and intermittent claudication. Relation between peripheral vascular complications and location of occlusive atherosclerosis in the legs, Acta Med Scand 1985;218(2): 217-21. Abstract.
- Jonason T, Ringqvist I. Factors of prognostic importance for subsequent rest pain in patients with intermittent claudication. Acta Med Scand 1985;218(1): 27-33. Abstract.
- American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care 2003;12:3333-41.
- Eneroth M, Apelqvist J, Troëng T, Persson BM. Operations, total hospital stay and costs of critical leg ischemia. A population-based longitudinal outcome study of 321 patients. Acta Orthop Scand. 1996 Oct;67(5):459-65.
- Jones WS, Patel MR, Dai D, et al. Temporal trends and geographic variation of lower-extremity amputation in patients with peripheral artery disease: results from U.S. Medicare 2000-2008. J Am Coll Cardiol. 2012 Nov 20;60(21):2230-6.
- Henry AJ, Hevelone ND, Belkin M, Nguyen LL. Socioeconomic and hospital-related predictors of amputation for critical limb ischemia. J Vasc Surg. 2011 Feb;53(2):330-9.
- Malone M, Lau NS, White J, et al. The effect of diabetes mellitus on costs and length of stay in patients with peripheral arterial disease undergoing vascular surgery. Eur J Vasc Endovasc Surg. 2014;48:447–451.
- Baubeta Fridh E, Andersson M, Thuresson M, et al. Impact of Comorbidity, Medication, and Gender on Amputation Rate Following Revascularisation for Chronic Limb Threatening Ischaemia. Eur J Vasc Endovasc Surg. 2018 Nov;56(5):681-688.
- Freisinger E, Malyar NM, Reinecke H, Lawall H. Impact of diabetes on outcome in critical limb ischemia with tissue loss: a large-scaled routine data analysis. Cardiovasc Diabetol. 2017 Apr 4;16(1):41.
- Spreen MI, Gremmels H, Teraa M, et al; PADI and JUVENTAS Study Groups. Diabetes is associated with decreased limb survival in patients with critical limb ischemia: pooled data from two randomized controlled trials. Diabetes Care. 2016 Nov;39(11):2058-2064.
- Shammas AN, Jeon-Slaughter H, Tsai S, et al. Major limb outcomes following lower extremity endovascular revascularization in patients with and without diabetes mellitus. J Endovasc Ther. 2017 Jun;24(3):376-382.
- Centers for Disease Control and Prevention. Hospital discharge rates for nontraumatic lower extremity amputation by diabetes status-United States, 1997. Morb Mortal Wkly Rep 2001; 50(43):954-8.
- Stratton IM, Adler AI, Neil HAW, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-12.
- Arya S, Binney ZO, Khakharia A, et al. High hemoglobin A(1c) associated with increased adverse limb events in peripheral arterial disease patients undergoing revascularization. J Vasc Surg. 2018 Jan;67(1):217-228.
- Takahara M, Kaneto H, Iida O, et al. The influence of glycemic control on the prognosis of Japanese patients undergoing percutaneous transluminal angioplasty for critical limb ischemia. Diabetes Care. 2010 Dec;33(12):2538-42.
- Ting W, Haskell L, Lurie F, et al. Impact of comorbid critical limb ischemia and diabetes on healthcare resource use and cost. PDB41 Abstract. Value in Health 2017;20(9) A481.
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005 Mar;86(3):480-6.
- Nejim B, Beaulieu RJ, Alshaikh H, et al. A unique all-payer rate-setting system controls the cost but not the racial disparity in lower extremity revascularization procedures. Ann Vasc Surg. 2018 Oct;52:116-125.
- Masoomi R, Shah Z, Quint C, Hance K, et al. A nationwide analysis of 30-day readmissions related to critical limb ischemia. Vascular. 2018 Jun;26(3):239-249.
- Conte MS, Bandyk DF, Clowes AW, et al. Results of PREVENT III; a multicenter, randomized trial of edifoligide for the prevention of vein graft failure in lower extremity bypass surgery. J Vasc Surg 2006;43:742-51.
- Sigvant B, Kragsterman B, Falkenberg M, et al. Contemporary cardiovascular risk and secondary preventive drug treatment patterns in peripheral artery disease patients undergoing revascularization. J Vasc Surg. 2016 Oct;64(4):1009-1017.
- Armstrong EJ, Ryan MP, Baker ER, et al. Risk of major amputation or death among patients with critical limb ischemia initially treated with endovascular intervention, surgical bypass, minor amputation, or conservative management. J Med Econ. 2017 Nov;20(11):1148-1154.
- Agarwal S, Sud K, Shishehbor MH. Nationwide trends of hospital admission and outcomes among critical limb ischemia patients: from 2003-2011. J Am Coll Cardiol. 2016 Apr 26; 67(16):1901-13.
- Armstrong EJ, Chen DC, Westin GG, et al. Adherence to guideline-recommended therapy is associated with decreased major adverse cardiovascular events and major adverse limb events among patients with peripheral arterial disease. J Am Heart Assoc. 2014 Apr 10;3(2):e000697.
- Conte MS, Bandyk DF, Clowes AW, et al. Risk factors, medical therapies and perioperative events in limb salvage surgery: observations from the PREVENT III multicenter trial. J Vasc Surg. 2005 Sep;42(3):456-64;discussion 464-5.
- Berger JS, Ladapo JA. Underuse of prevention and lifestyle counseling in patients with peripheral artery disease. J Am Coll Cardiol. 2017 May 9;69(18):2293-2300.
- Agarwal S, Pitcavage JM, Sud K, Thakkar B. Burden of readmissions among patients with critical limb ischemia. J Am Coll Cardiol. 2017;69:1897–1908.
- Secemsky EA, Schermerhorn M, Carroll BJ, et al. Readmissions after revascularization procedures for peripheral arterial disease: a nationwide cohort study. Ann Intern Med. 2018 Jan 16;168(2):93-99.
- Vahidy FS, Donnelly JP, McCullough LD, et al. Nationwide estimates of 30-day readmission in patients with ischemic stroke. Stroke. 2017 Jan 1:STROKEAHA-116.
- Fingar K. (Truven Health Analytics), Washington R (AHRQ). Trends in Hospital Readmissions for Four High-Volume Conditions, 2009–2013. HCUP Statistical Brief #196. November 2015. Agency for Healthcare Research and Quality, Rockville, MD. [Internet. Accessed 2019, May.] Available at:
http://www.hcup-us.ahrq.gov/reports/statbriefs/sb196-Readmissions-Trends-High-Volume-Conditions.pdf. - Bodewes TC, Soden PA, Ultee KH, et al. Risk factors for 30-day unplanned readmission following infrainguinal endovascular interventions. J Vasc Surg. 2017;65:484–494.e3.
- Reed GW, Raeisi-Giglou P, Kafa R, et al. Hospital readmissions following endovascular therapy for critical limb ischemia: associations with wound healing, major adverse limb events, and mortality. J Am Heart Assoc. 2016;5:e003168.
- Berger A, Simpson A, Bhagnani T, et al. Incidence and cost of major adverse cardiovascular events and major adverse limb events in patients with chronic coronary artery disease or peripheral artery disease. Am J Cardiol. 2019 Mar 16. pii: S0002-9149(19)30319-4. doi: 10.1016/j.amjcard.2019.03.022. [Epub ahead of print]
- Looser PM, Feldman DN. Thirty-day readmissions for critical limb ischemia: ready for a new quality metric? Circulation. 2017;136:177–179.