CASE #3:
History and Symptoms
A 68-year-old male with a long history of extensive atherosclerosis presented with left leg ischemic rest pain of a few weeks’ duration. The patient had prior remote bilateral iliac artery stenting, failed lower extremity bilateral Fem-Pop bypass and CFA endarterectomy, and remote right-to-left femoral-femoral (Fem-Fem) bypass for left iliac stent occlusion.
An angiogram showed patent aorta, as well as right common and external iliac stents. Left common iliac and left external iliac had stents and known CTO. The Fem-Fem bypass was occluded. The left CFA was also occluded with patent left profunda and occluded left SFA.
Procedure Highlights
It was a technically difficult procedure requiring 5 hours, with the first 2.5 hours spent declotting the Fem-Fem bypass without success through right femoral access.
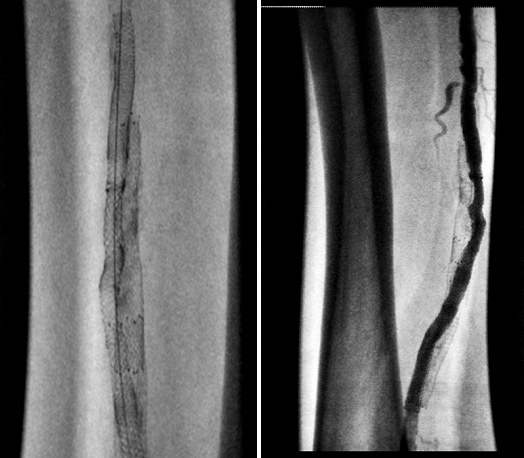
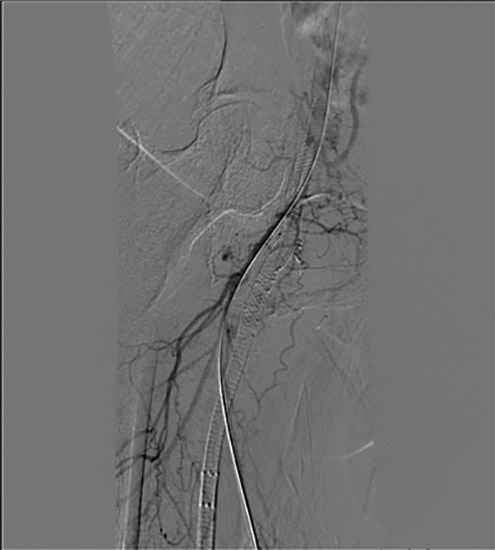
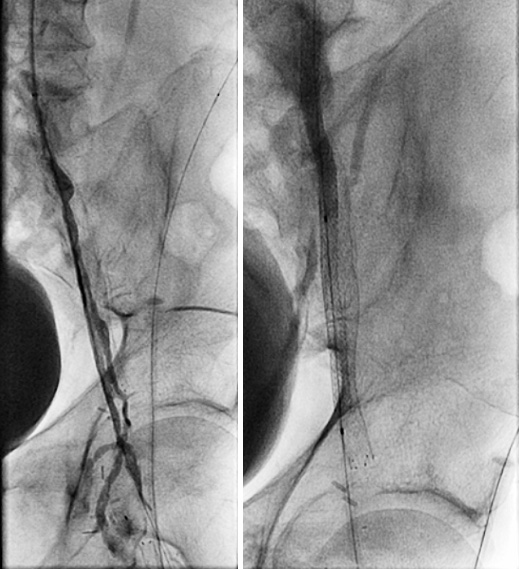
We then obtained access in the left brachial artery, with additional access in a retrograde fashion in the left profunda femoris. We successfully crossed the contiguous CTO of the left common iliac and left external iliac, as well as the left common femoral artery. The left iliac segment stent long CTO crossing would only occur outside the existing occluded stent. We conservatively carried out angioplasty of the iliac segment with progressively larger balloons to avoid vessel rupture. The patient was kept lightly sedated with frequent questioning about any pain and rigorous hemodynamic monitoring. Despite good balloon expansion, there was, as expected, severe recoil necessitating double-barrel stenting of the new lumen.
We chose bare metal stents to keep the sheath size small in the diffusely diseased brachial and profunda. We stented the left common iliac and left external iliac artery using a combination of a 6×58 Omnilink and 5×58 Omnilink, respectively, and the left CFA using an 8×80 Absolute stent covering the entire length of the vessel (CFA was de-novo stenting).
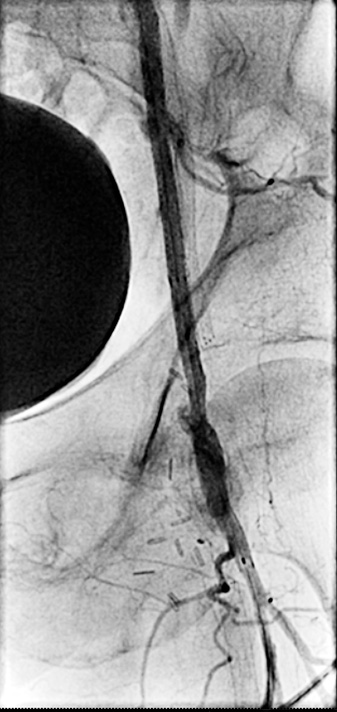
Final angiographic findings were that the left CFA, common iliac, and external iliac reduced to less than 20% with well-deployed stents. The left SFA was totally occluded with good flow into the left profunda femoris, which then collateralized at the popliteal.
The patient tolerated the procedure well and had immediate relief of his rest pain, with only claudication at a moderate distance that was not lifestyle-limiting.
Timeline
Jan. 2012: Index procedure
March 2015: Angiogram shows ISR, treated with PTA for secondary patency
April 2019: Angiogram follow-up shows patent iliac stents